How U.S. Healthcare Really Broke: An Incentives Framework
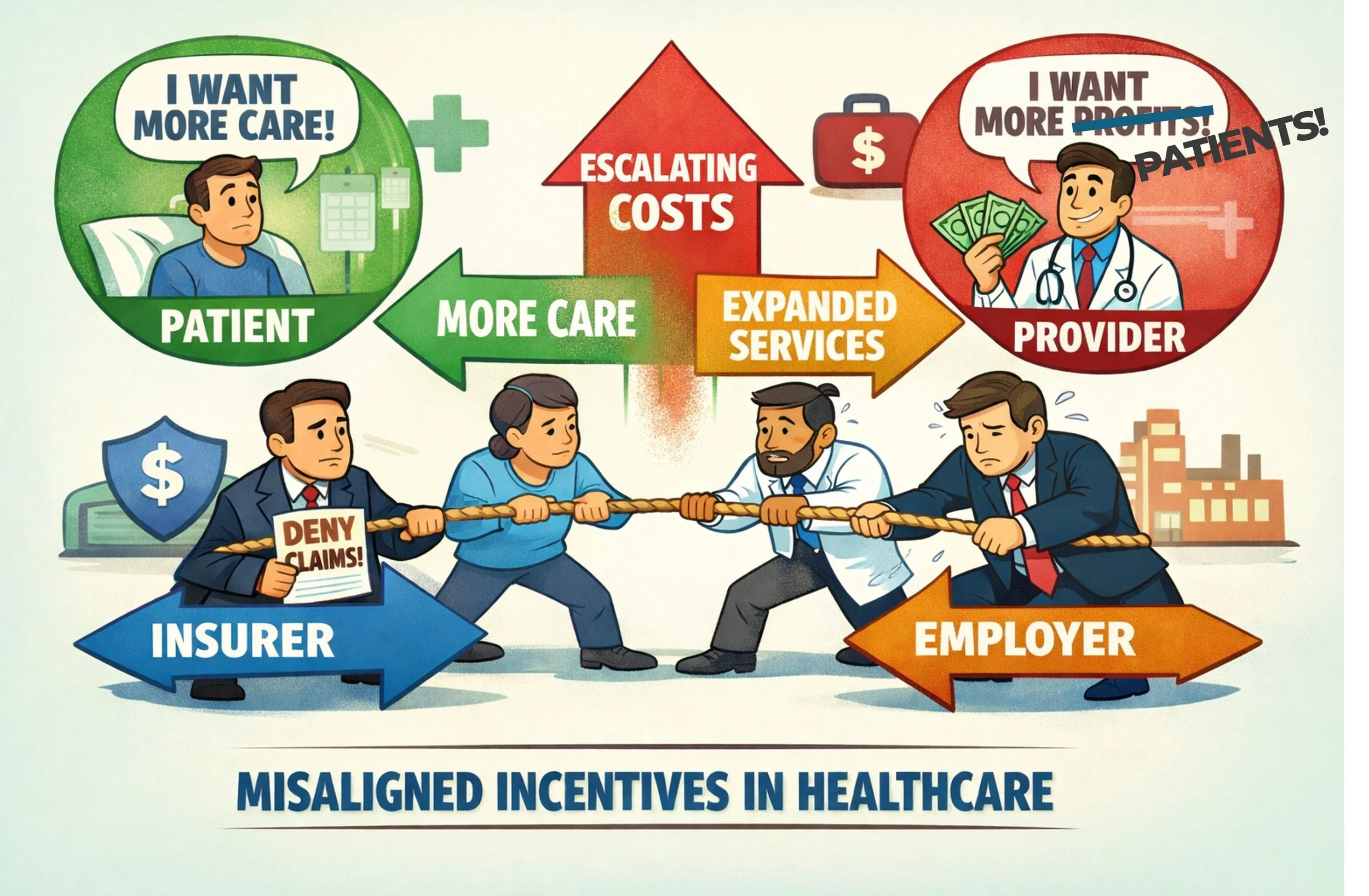
Most healthcare explanations lean on ideology or emotion. Here we examine incentives - how rules, markets, and institutions combine to produce higher costs and growing complexity.
The Goal: Establish criteria to make something better.
What happens when healthcare ideas meet real people, real incentives, and real limits? This paper provides the framework to give the answer.
Instead of judging policies by how they sound on paper or from a microphone, it examines how human behavior and the limitations of time and money shape what actually happens. The goal is to have every healthcare system proposal stress-tested through the same criteria to see whether its promised outcomes are achievable in the real world.
Healthcare Discussion Topics
Sample sections are below: Learn how they combine to paint the full picture of U.S. healthcare in the complete document.